

Abdominal Examination For OS4.
Exam Flow:
- Inspection of the hands, face, tongue, chest and neck.
- Radial pulse.
- Palpation. – The 5 F’s.
- + AAA.
- + Superficial palpation.
- Auscultation.
- Palpation.
- + Deeper palpation – organomegaly.
- + Liver.
- + Spleen.
- + Kidneys.
- + Bladder. (optional).
- + Deeper palpation – organomegaly.
- Percuss.
Inspection of the hands, face, eyes, tongue, neck and chest:
- First of all, have the patient seated on the couch, laying down – exposed from the waist up. Throughout this exam, always keep in mind the 5 F’s:
- Fat.
- Fluid.
- Fetus.
- Flatus. (Gas).
- Faeces.
Hands:
- Koil-onychia:
- Also known as spoon nails, is a nail disease that can be a sign of hypochromic anaemia, especially iron-deficiency anaemia.
- Leuk-onychia:
- Known as white nails or milk spots, is a medical term for white discoloration appearing on nails. Due to air bubbles present between the nail and its bed. Also Hypoalbumineamia.
- Clubbing:
- An abnormal widening and thickening of the finger tips and nails.
- + Crohn’s disease. (Type of inflammatory bowel disease (IBD) that may affect any part of the gastrointestinal tract from mouth to anus, commonly effecting the colon and ileum. Associated with ulcers and fistulae).
- + Ulcerative colitis. (A form of inflammatory disease (IBD) of the colon, the largest part of the large intestines. That includes characteristic ulcers, or open sores).
- + Coeliac disease. (Small intestine is hypersensitive to gluten, leading to difficulty in digesting food).
- To test for clubbing, use the Schamroth’s Window Test.
- Asterixis (Flapping tremor):
- Quite slow frequency, whole hand tilts forwards – a result of encephalopathy (brain function disease) caused by urea.
- Palmar erythema:
- A reddening of the thenar and hypothenar eminences.
- “Corn Beef Hands”.
- Chronic liver disease.
- Pregnancy.
- Nicotine staining.
- Dupuytren’s contracture:
- Alcoholic liver disease.
- Known as Vikings Disease.
- Is a connective tissue disorder – a fixed flexion contracture of the hand due to palmar fibromatosis (refers to a group of benign (non-harmful) soft tissue tumours).
Eyes:
- Check the conjunctiva (mucous membrane that covers the front of the eye and lines the inside of the eyelids) to check for Pallor –> anaemia.
- Check the Sclera (White outer layer of the eyeball) for jaundice (excess pigment bilirubin and typically caused by obstruction of the bile duct, liver disease, or excessive breakdown of RBC’s).
- Xanthelasma.
Mouth:
- Patient opens, look at the inside of the mouth, inside of cheeks for any ulcers –> Chron’s disease (Type of inflammatory bowel disease (IBD) that may affect any part of the gastrointestinal tract from mouth to anus, commonly effecting the colon and ileum. Associated with ulcers and fistulae).
- Look at the tongue.
- + Fat and red = possible sign of anaemia.
- Side of the mouth where the lips meet.
- + Angular Stomatitis, Inflammation corners of the mouth commonly unilaterally but can be bilateral. Commonly linked to candidiasis (oral thrush).

Neck:
- Palpate the Virchow’s Node in the upper left supraclavicular fossa, this node drains the thoracic duct. Enlargement or Troisier’s sign may suggest metastatic cancer from either the abdomen or lungs.
Radial Pulse Check:
- There is some argument as to whether this should be performed or not in an abdominal exam.
- Good indicator of Sepsis (Harmful bacteria and their toxins in tissue) or Thyroid Disease.
- Rate or bounding.
- Rate is increased with asthma patients.
- At the wrist, lateral to the flexor carpi radialis.
- Three fingers over one artery, assess rate, rhythm and volume.
- Count over 15 seconds and multiply by 4.
- Then palpate both radial pulses at the same time to assess volume differences.
- Palpate the radial and ipsilateral femoral pulse (radio-femoral delay).
Next step is to get the patient to lay down flat on the couch from the currently seated position.
Chest:
- Spider Naevi. A cluster of minute red blood vessels visible under the skin, occurring typically during pregnancy or as a symptom of certain diseases (e.g. Alcoholic cirrhosis, Liver cirrhosis but can be caused by any condition that results in increased levels of oestrogen). 5 or more = significant.

- In males, check for Gynaecomastia: (Enlargement of a man’s breasts. Hormone imbalance).
- Both of these are characteristics of Liver Pathology.
Now just have a general over look of the abdomen:
- Scars.
- Masses.
- Pulsations.
- Abdominal distension – fluid/air that has built up to go beyond the normal girth of the stomach and waist. Underlying disease or dysfunction in the body rather than an illness in its own right. “Bloated Feeling”.
Auscultation:
- Auscultation for bowel sounds may be carried out before percussion and palpation due to adverse effect that these procedures may have on the sound from the bowels.
- Listen with the diaphragm around the quadrants for up to 30 seconds.
- Listen for arterial bruits over the aorta. They may also arise from stenosis of renal arteries.
- Listen for friction rubs over liver and spleen.
- High pitched may indicate bowel obstruction. Sounds like water being poured from one cup to another.
- Absence of sounds may be also be caused by peritonitis (inflammation of the peritoneum).
Palpation:
- Firstly palpate the abdominal aorta checking for AAA.
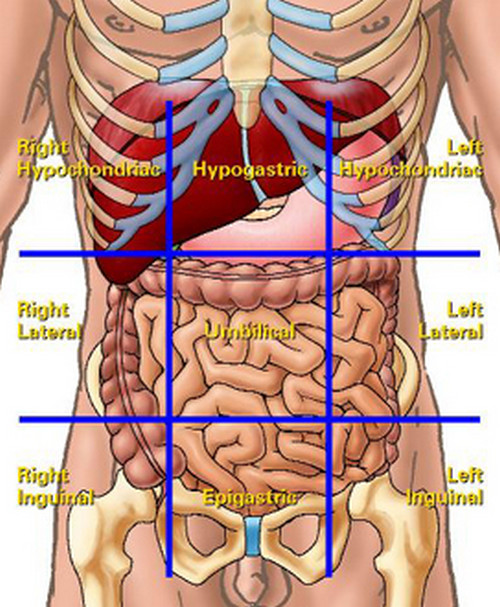
- Palpation of the abdomen should be performed in a systematic way using the 9 named segments of the abdomen:
- + Right and left hypochondrium,
- + Right and left lumbar flanks,
- + The umbilical area,
- + The hypogastric,
- + The right and left iliac regions.

- Initial examination should be superficial using one hand. Place the hand flat over each area and flex at the metacarpophalangeal joints. You should feel whether the abdomen is soft but you should always be looking at the patient’s face for any signs of pain. – hedgehog hand.
- Once all 9 areas have been examined superficially, you should move on to examine deeper.
- A deeper exam is performed with two hands, one on top of the other again flexing at the MCP joints.
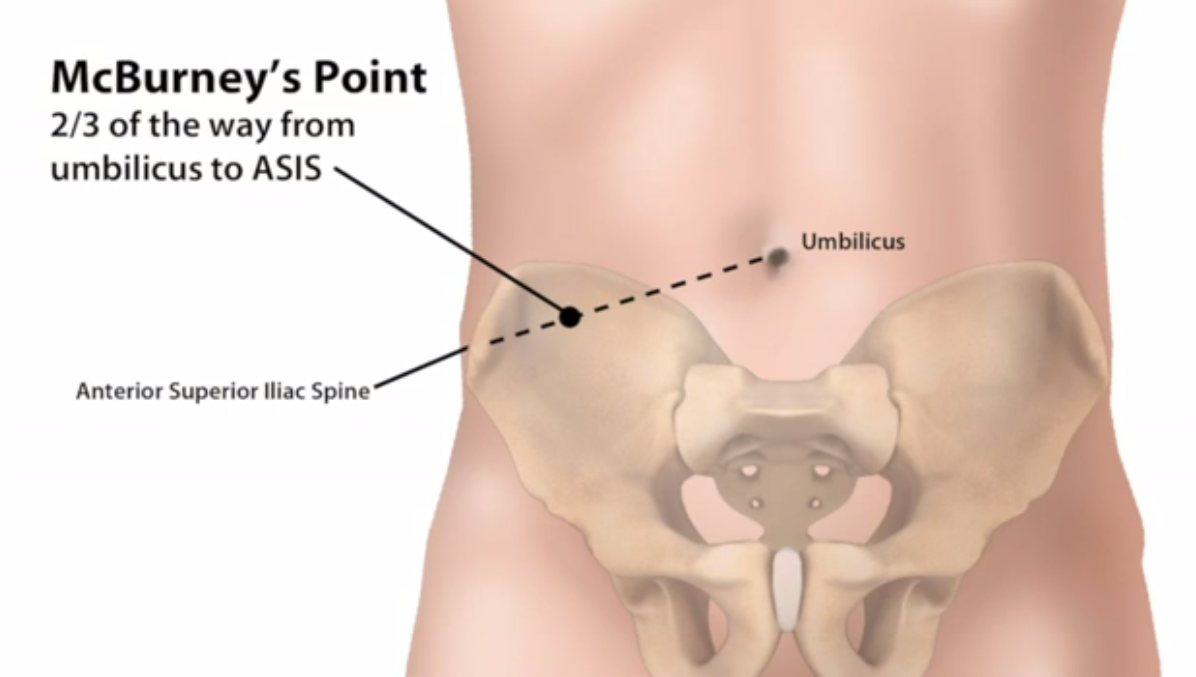
- Use Mc’Burney’s Point, add pressure, if pain = possibility of appendicitis.

- Murphy’s sign can be elicited by placing your examining fingers over the gallbladder area and then asking the patient to take a deep breath.
- If Murphy’s sign is positive, there will be sudden reaction of the pain on inspiration and inspiration will be inhibited.

Organomegaly:
Liver, Spleen and Kidneys:
- Palpation for the liver and spleen is similar, both starting in the right iliac fossa.
- For the liver: press upwards towards the right hypochondrium. You should try to time the palpation with the patient’s breathing – in as this presses down on the liver If nothing is felt you should move towards the costal margin. Should feel soft but firm. (Fish tongue).
- Palpating for the spleen: Start well below the left costal margin. Ask patient to breath deeply, feel for splenic edge as it descends on inspiration. Not normally palpable.
- To feel for the kidneys: Right lower than Left. General population can’t be palpable. Place one hand under the patient L1/L2 in the lateral region and the other hand on top. You should then try to bring the kidney between the two hands by bring up the inferior hand and pushing the superior hand down. In the majority of people the kidneys are not palpable, but they maybe in thin patients who have no renal pathology.
- Kidney palpation can also be done seated too. Palpate the renal angle for tenderness. Gently percuss with closed fist “Kidney Punch.”


Percussion:
- Percussion over the abdomen is usually resonant (deep and clean sound), if there is a dull sound it usually means solid or liquid.
- Percussion allows you to determine if abdominal distension is because of solid or cystic tumours, ascites (the accumulation of fluid in the peritoneal cavity, causing abdominal swelling), or gas.
- Fullness of the flanks may be the first indication of ascites.
- Percussion for shifting dullness:
- Supine. Percuss from the umbilical region moving down towards one side.
- When the sound becomes dull, mark the spot (or keep your finger there) and ask the patient to move on to the opposite side. Give a short while for the fluid to sink and percuss again.
- If the marked spot now becomes resonant that is a positive sign of ascites .
- Percuss back down towards the umbilicus until dullness is reached again. Repeat on the other side.
- Eliciting a fluid thrill:
- With one hand on the patient’s flank, flick the skin over the other flank using a finger. If an impulse or ‘fluid thrill’ is felt, this indicates a positive sign.
- However, to be certain, you should repeat the examination with the patient’s hand along their midline in the sagittal plane to dampen any possible thrill transmitted by the abdominal wall.
It can be considered to do that auscultation part of this exam again, to check for possible changes in the gut due to all of the previous changes.
